Effects of the Whole-Body Cryotherapy on a Total Antioxidative Status and Activities of Some Antioxidative Enzymes in Blood of Patients with Multiple Sclerosis Preliminary Study
Abstract:
Objective. There is evidence that multiple sclerosis (MS) is not only characterized by immune mediated inflammatory reactions but also by neurodegenerative processes. Neutralization of oxidative stress and excitotoxicity, might represent a therapeutic approach to provide neuroprotection in MS. The purpose of this study was to compare changes in total antioxidative status and activities of chosen antioxidative enzymes, such as : SOD, CAT in erythrocytes of patients with MS before and after using WBCT with control group. Materials and methods. 32 patients with multiple sclerosis (ICD10-G35) and 20 healthy subjects were recruited for the study. The examined MS group (n=16) was treated with a series of 10 daily exposures in a cryogenic chamber (2-3 min, from -120!- ! to -110!- !) and program of exercises. The control MS group (n=16) had only exercises. Plasma TAS as well as SOD and CAT activities in erythrocytes were measured. Results. The level of TAS in MS patients was distinctly reduced compared to healthy subjects. After two weeks of WBCT treatment an increase of TAS in the whole examined group (p 0,01) were observed in relation to control MS group. There was not increase of CuZnSOD and CAT activities. Conclusion. Our results suggest positive antioxidant effects of WBCT as a short-term adjuvant treatment for patients suffered due to MS. J. Med. Invest. 57 : 168- 173, February, 2010
Keywords : antioxidants, multiple sclerosis, whole-body cryotherapy
INTRODUCTION
Accumulating data indicate that oxidative stress (OS) plays a major role in the pathogenesis of multiple sclerosis (MS). Reactive oxygen species (ROS), leading to OS, generated in excess primarily by macrophages, have been implicated as mediators of demyelization and axonal damage in MS. ROS cause damage to main cellular structures and components such as lipids, proteins and nucleic acids (e. g., RNA, DNA), resulting in cell death by necrosis or apoptosis. In addition, weakened cellular antioxidant defense systems in the central nervous system (CNS) in MS, and its vulnerability to ROS effects may augmented damage (1). Thus, treatment with antioxidants might theoretically prevent propagation of tissue damage and improve both survival and neurological outcome. Hypothermia has long been known as a potent putative neuroprotectant. It delays energy depletion, reduces intracellular acidosis and ischemia, related to the accumulation of excitotoxic neurotransmitters, and attenuates the influx of intracellular calcium. Additionally, hypothermia inhibits production of oxygen free radicals involved in the secondary damage, associated with reperfusion. It also suppresses mechanisms of blood-brain barrier degeneration and postischemic remodeling (2-4). Treatment using total immersion of the body in extremely low temperatures was first introduced in Japan towards the end of the 1970s by Yamauchi T (5) who constructed the first cryogenic chamber and successfully used cryotherapy to treat rheumatism. We considered that the effects of whole body cryotherapy (WBCT) exposures could be associated with increasing of antioxidative system, therefore the purpose of this study was to compare the effects of WBCT on changes in total antioxidative status (TAS) of plasma and activities of the chosen antioxidative enzymes in the erythrocytes of patients with MS, such as superoxide dismutase (SOD) and catalase (CAT).
CASE REPORT
Patients presentation Inclusion/exclusion criteria for this study were a diagnosis of MS and the ability to ambulate independently. Patients with such conditions as : circulatory or breathing insufficiency, clotting, embolism, inflammation of blood vessels, open wounds, ulcers, serious cognitive disturbances, fever, addictions, claustrophobia, and over-sensitivity to cold were excluded from the study. The subjects (n=32) received no hormones, vitamins, minerals or any other substitutions with antioxidative properties. None of the subjects had previously used WBCT. Prior to the study, all the subjects had undergone medical check-ups including neurological and internistic examination. The subjects were randomized into two groups (16 subjects in each). Both groups were treated by program of exercises. This includes a 20-30 min program of progressive balance and muscle strengthening exercises. All sessions included 5 minutes warm-up exercises. The examined group had participated additionally to WBCT sessions. 20 healthy volunteers were chosen to the study as a control to MS. The protocol and procedures were done according to the Helsinki Declaration and were approved by Ethics Committee of the Medical University of Lód!”, Poland. The study was performed in the Department of Biochemistry and Rehabilitation Division III General Hospital in Lód!”.
Experimental design
An experimental trial (WBCT) consisted of the 16 subjects treated by a cycle of 10 exposures in a cryogenic chamber carried out daily from Monday to Friday. The cryogenic chamber has two rooms : the vestibule, with the temperature of -60!#, and the main chamber, with temperature between -110!# and -160!#. Liquid nitrogen is used as the coolant. Sessions in the chamber lasted 2-3 min. Gregorowicz and Zagrobelny (6) provide guidance on the appropriated duration of exposure and temperature for adult patients as well as a list of medical conditions in which WBCT is unsuitable. The study was carried out in the spring 2008. Observations were made in 3 groups : I-MS patients treated by kinesytherapy, II-MS patients immersed by WBCT and kinesytherapy and III-healthy volunteers. MS patients were examined at 2 stages : at the beginning of the treatment and at the end. Healthy subjects had one examination. Blood samples were collected in cooled EDTA tubes centrifuged to isolate plasma and erythrocytes. The specimens were taken one hour before the 10 days cycle of therapy and one hour after the last immersion in both MS groups.
Biochemical investigations
Total Antioxidant Status (TAS) was measured in plasma samples (healthy group and MS patients) using the kit by Randox Laboratories Ltd.(Cat. No. NX 2332). The plasma volume taken to estimation was 5 µl, a total assay volume was 305 µl. The reaction was carried out during 3 min. And measured spectrophotometrically at 600 nm. The activities of antioxidative enzymes were determined in erythrocytes. Superoxide dismutase activity in erythrocytes was The Journal of Medical Investigation Vol. 57 February 2010 169 measured according to Misra and Fridovich (7) methods. The absorbance of the examined samples was estimated at 380 nm using Becman spectrophotometer at 37!!. The activity was expressed as U/g Hb. Catalase activity in erythrocytes was determined according to Beers and Sizer method (8). Absorbance was measured at 240 nm using Becman spectrophotometer. Enzymatic activity was expressed as Berg Mayer units U/gHb.
Statistical analyses
Results were statistically elaborated. Due to nonparametric distribution the Wilcoxon test was used to analyze changes. Results were compared with healthy subjects.
Results of TAS measured in mM were considered statistically significant (p”0,01) whereas CAT activity decreased. The results in both groups were uniform.
Results
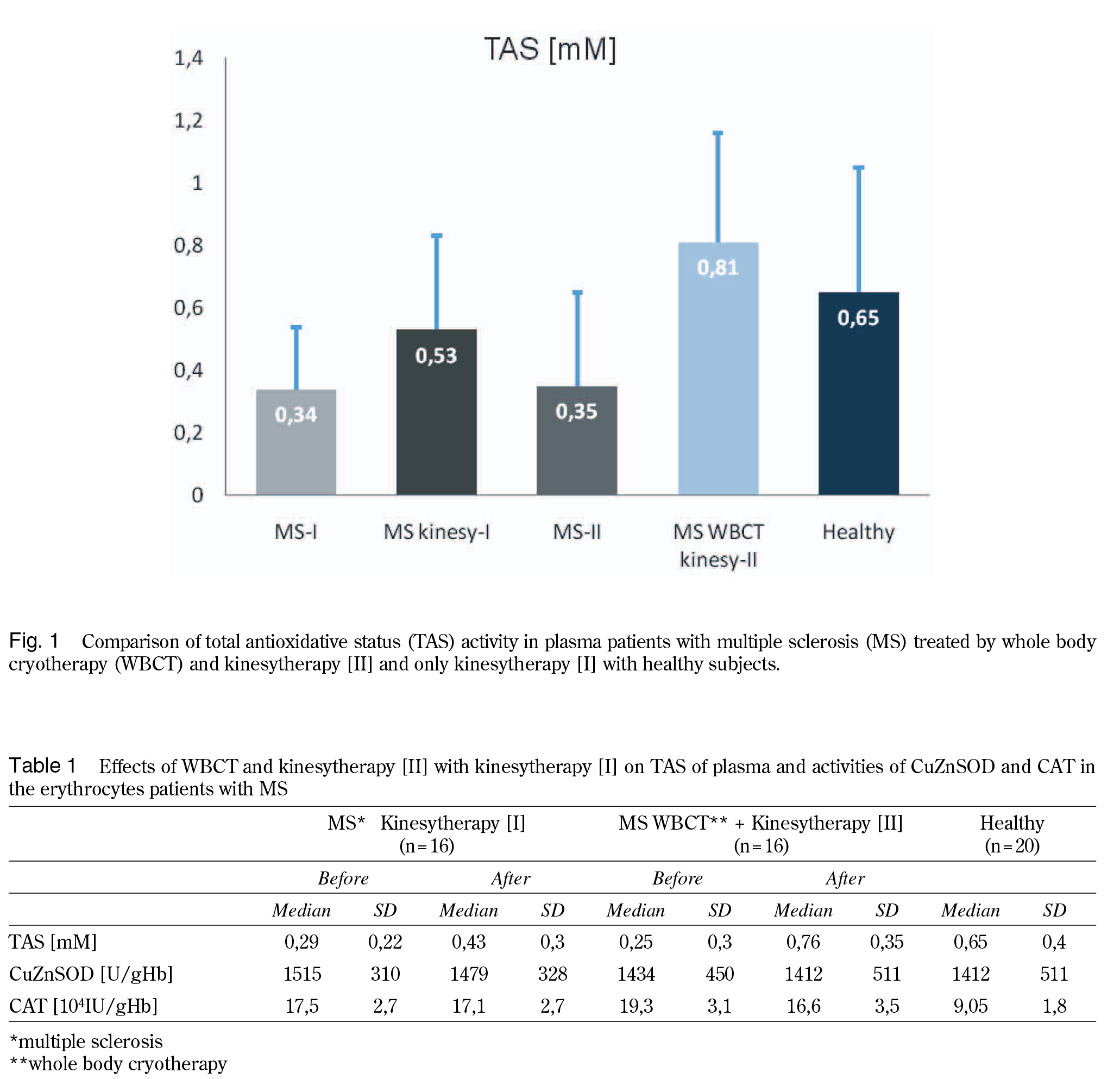
Our studies have shown that the level of TAS in MS patients is distinctly reduced compared to healthy subjects (Fig. 1). WBCT caused statistically significant increase of TAS in plasma of MS patients (α=0,001) (from 0,3468 mM to 0,8126 mM) compared to non WBCT MS patients (from 0,3427 mM to 0,5266 mM) (Fig. 1 Table 1).
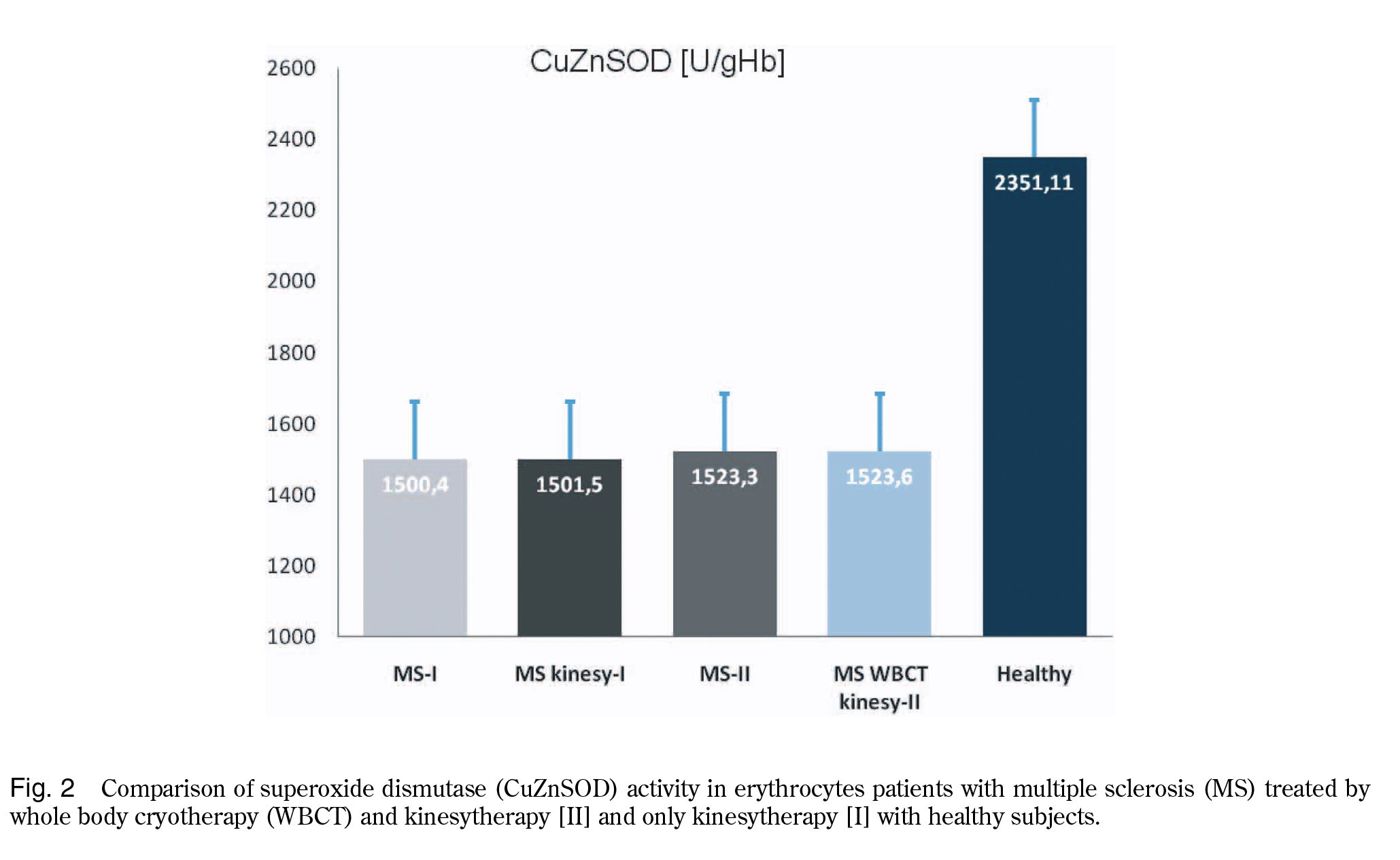
In erytrocytes of MS patients the level of SOD activity is significantly reduced compared to healthy group (Fig. 2).
We have observed that activity of CuZnSOD in erythrocytes of MS patients after WBCT treatment was not statistically significant change (Fig. 2 Table 1).
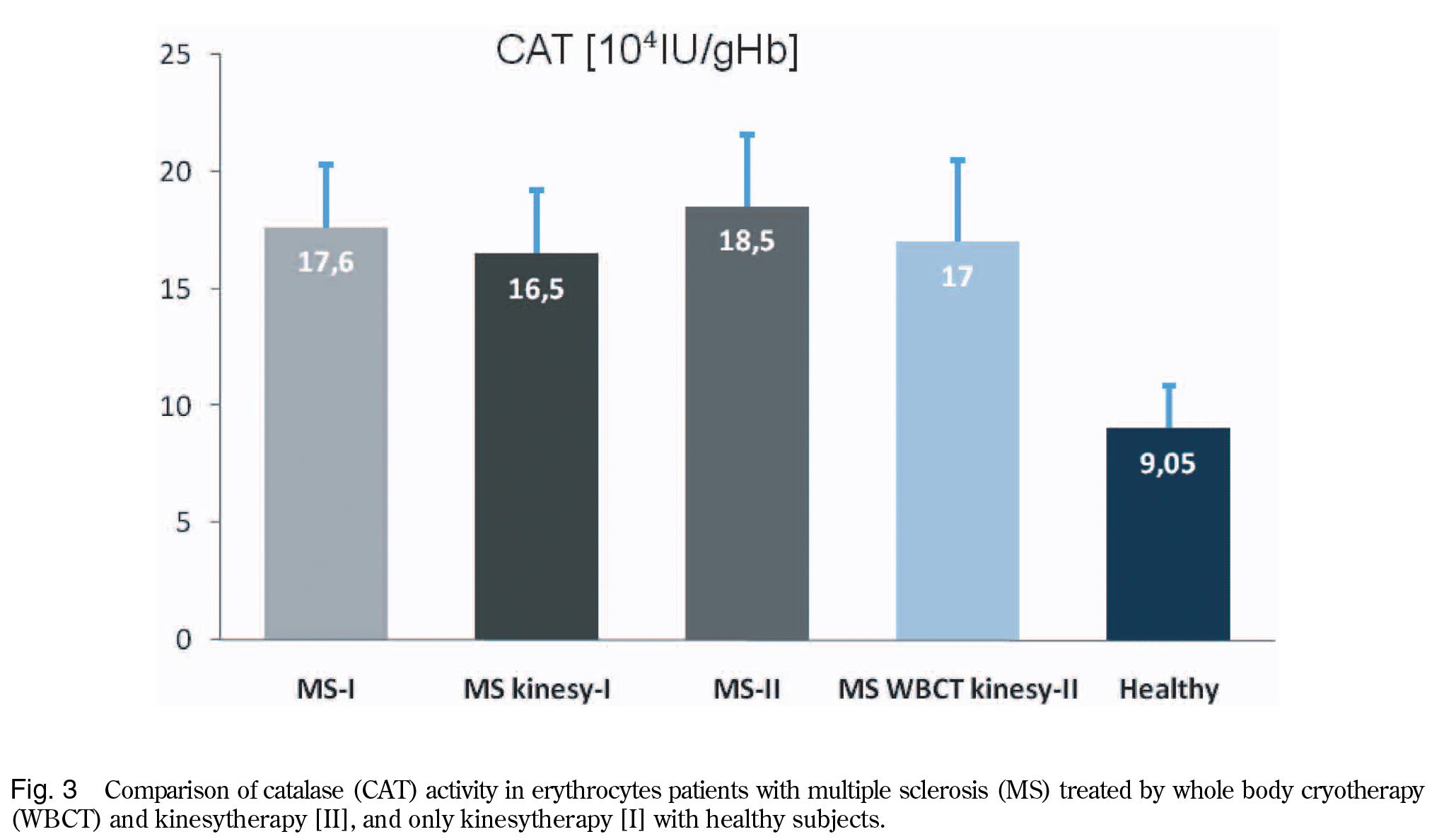
Contrary to activity SOD, activity of CAT was distinctly (2-fold) higher in erythrocytes of MS patients than in healthy volunteers and exercise therapy had no effect on CAT activity (Fig. 3 Table 1).
DISCUSSION
Oxidative stress is a hallmark of neuregenerative disorders MS symptomatology and complications of its negative symptoms. OS could be caused by prolonged altered metabolism, exposure to exogenous oxidizing agents or compounds and it has been tied to inflammatory response.
The antioxidant defense system in the organism comprises enzymatic and non enzymatic components. The enzymatic antioxidant system includes a variety of antioxidant enzymes such as SOD, CAT, GPx. We observed that MS patients the activities of erythrocyte antioxidative enzymes, specially SOD is distinctly reduced (contrary to CAT) (Fig. 2, 3).
Antioxidants, whether synthesized endogenously or exogenously administered are reducing agents that neutralize the oxidative compounds (ROS) before they can cause damage to different biomolecules.
The measurement of TAS in plasma represents the body redox status better than does measure of the single circulating antioxidant.
After strenuous physical exercise, a significant increase in TAS may occur (9). We observed that after exercise MS patients TAS in plasma was increased compared to untreated patients.
The present data demonstrate that plasma TAS was found to be significantly lower in MS patients than in healthy group (Fig. 1). This findings indicate that an impaired antioxidant defense system that may be dependent partly on lower activity of SOD. It seems that the observed low level of TAS in plasma of MS patients may be also dependent on the low concentrations of endogenous antioxidants, mainly uric acid. In humans, over half the antioxidant capacity of blood plasma comes from uric acid. It is known that the lower values of uric acid (!194 µmol/l) have been associated with MS, whereas serum uric acid in healthy subjects was !290 µmol/l. MS patients in remission reach the level of uric acid about 230 µmol/l. Uric acid like ascorbic acid are strong reducing agents and potent antioxidant (10).
It should be emphasized that despite lowering activities of CuZnSOD and CAT the total antioxidative status significantly increased from 0,3468 mM to 0,8126 mM. Maybe that other antioxidantive enzymes or non enzymatic substances like GSH, glutamate reductase, vitamins, microelements that can also affect this fenomenon.
There are evidences that both cryotherapy and moderate exercises cause increase in antioxidant status (9-12). Similar results were found in the study performed by Duque, et al. (13) in which mean TAS value significantly increased 2 minutes after the exposure to cold in the healthy man group treated with WBCT.
Siems, et al. (14) investigated the effects of the acute cold stimuli (winter swimming) on a number of oxidative stress markers and showed that these stimuli induced a decrease in the concentration of several major plasma antioxidants (i.e. ascorbic acid, uric acid) (14). In addition, erythrocyte level of oxidized glutathione and the ratio of oxidized glutathione/total glutathione also increased following the cold exposure (15). The authors also indicated the higher enzymatic protection (i.e.changes in the activities of red blood cells catalase, glutathione peroxidase, superoxide dismutase) in healthy individuals regularly practicing winter swimming activities compared with control subjects (16).
If protection against oxidative stress due to WBCT treatment develops, increase in the values of TAS observed after the exposures to cold stress should reach the values observed in healthy subjects.
The obtained results suggest that cryotherapy may play an important role in the process of activation of antioxidative properties in MS patients, since the increase in the TAS was considerably greater after using WBCT than after physical exercise.
WBCT is worth of particular concern in treatment of patients with MS because of safety of used procedure, minimal side effects.
CONCLUSION
Our observations showed that WBCT resulted in the increase of TAS ten days after the exposure.
ACKNOWLEDGEMENTS
We thank Juha Oksa, Ph.D., Adjunct Professor Finnish Institute of Occupational Health, Oulu Centre of Expertise for Health and Work Ability Physical Work Capacity team for possibility of known with his articles.
REFERENCES:
1. Gilgun-Sherki Y, Melamed E, Offen D : The 172 E. Miller, et al. Antioxidant effect of whole body cryotherapy multiple sclerosis role of oxidative stress in the pathogenesis of multiple sclerosis. The need for the effective antioxidant therapy. J Neurol 251 : 261-8, 2004
2. Muniandy S, Qvist R, Ong SYG, Bee CH, Koon CY, Rayappan A : The oxidative stress of hyperglycemia and the inflammatory process in endothelial cells. J Investigating Med 56 : 6-10, 2009
3. Gonsette R : Oxidative stress and excitotoxicity : a therapeutic issue in multiple sclerosis? Mult Scler 14 : 22-34, 2008
4. Liu L, Yenari M : Therapeutic hypotheramia : neuroprotective mechanisms. Front.Biosci 12 : 816-25, 2007
5. Yamauchi T : Whole body cryotherapy is method of extreme cold -175!!treatment initially used for rheumatoid arthritis. Z Phys Med Baln Med Klin 15 : 311, 1989
6. Gregorowicz H, Zagrobelny Z : Systemic cryotherapy. Indications and contraindications, its course, and physiological and clinical results. In : Podbielska H, Str k W, Miller G, eds. Acta biomedical Engineering. Whole body cryotherapy. Indygo Zahir Media, 2007, pp 4-16.
7. Mirsa HP, Fridovich J : The role of sueroxide anion in the autooxidation of epinephrine and a simple assey superoxide dismutase. J Biol Chem 247 : 3170-3175, 1972
8. Beers R, Sizer T : A spectrophotometric method for measuring the breakdown of hydrogen peroxide by catalase. J Biol Chem 195 : 133-140, 1952
9. MacKinnon K, Molnar Z, Lowe D, Watson I, Shearer E : Measures of total free radical activity in critically ill patients. Clin Biochem 32 : 263-268, 1999
10. Massa J, O’Reilly E, Munger KL, Delorenze GN, Ascherio A : Serum uric acid and risk of multiple sclerosis. J Neurol : 2009 (Epub ahead of print)
11. Meyer-Heim A, Rothmaier M, Weder M, Kool J, Schenk P, Kesselring J : Advanced lightweight cooling-garment technology : functional improvements in thermosensitive patients with multiple sclerosis. Mult Scler : 13 : 232-7, 2007
12. Leppaluoto J, Westerlund T, Huttutnen P, Oksa J, Smolander J, Dugue B : Effects of long- term whole-body cold exposures on plasma concentrations of ACTH. Beta-endorphin, cortisol, catecholamines and cytokines in healthy females. Scand J Clin Lab Invest 68 : 145-153, 2008
13. Duque B, Smolander J, Westerlund T, Oksa J, Nieminen R, Moilanen E, Mikkelsson M : Acute and long-term effects of winter swimming and whole-body cryotherapy on plasma antioxidative apacity in healthy women. Scand J Clin Lab Invest 65 : 395-402, 2005
14. Siems W, Van Kuuk F, Maas R, Brenke R : Uric acid and glutathione levels during shortterm whole body cold exposure. Free Radical Biol Med 16 : 299-305, 1994
15. Siems W, Brenke T : Changes in the glutathione system of erythrocytes due to enhanced formation of oxygen free radicals during short- term whole body cold stimulus. Arct Med Res 51 : 3-9, 1992
16. Siems W, Brenke R, Sommerburg O, Grune T : Improved antioxidative protection in winter swimmers. Q J Med 99 : 193-8, 1999